
Anterior Cruciate Ligament
Anterior cruciate ligament (ACL) injuries are very common. They affect people from aged 12 upwards and are common among people who play sports, especially football, netball, rugby and skiing.
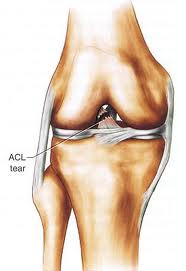
The ACL is a thick ligament running through the centre of each knee. It provides stability against rotation and excessive movement of the femur (thigh bone) on the tibia (shin bone). It also sends important information to the brain about balance and control and where the knee is in space during all activities.
An ACL rupture usually occurs in a non contact injury where the leg tries to twist but the foot stays stuck to the ground. It is also commonly occurs when landing awkwardly on one leg for example after jumping for a header in football. ACL ruptures are also often seen in rugby and netball players and skiers.

- The person will often report hearing or feeling a ‘pop’ sensation at the time of the injury.
- Pain. Ranging from mild to very severe.
- Swelling. Occurs almost immediately due to the blood released into the knee joint when the ligament tears. In some cases swelling does not appear which is why accurate assessment is essential.
- Giving way. This is extremely common long term especially in cases where the diagnosis of ACL tear has been delayed.

When the ligament is torn it cannot repair itself. In many cases it is possible to compensate for this tear by strengthening and improving the balance and control of the muscles around the knee. This is best achieved under the guidance of a physiotherapist, as the exercises are very specific.
If conservative treatment is not successful or if the patient is a high level sportsperson then surgery may be the best option. The ligament is replaced by a graft that is made out of a section of the patient’s own hamstring muscles (semimembranosus and semitendonosus) or the patella tendon. The rehabilitation after surgery is very important, as although the graft is very strong it needs the support and control of the muscles and receptors in and around the knee to ensure long tern function.
